The 2026 Power-Couple Therapy Avoidance Report
An analysis of why, in 63% of dual-high-achievement couples, neither partner has ever entered therapy individually or as a couple, and what the shared avoidance costs the relationship.

Dual-high-achievement couples (where both partners hold senior professional roles, founder positions, or equivalent achievement status) show a distinctive pattern at intake: in 63% of CEREVITY's couples cohort, neither partner has ever entered therapy individually or together prior to the couple's first contact with the network. The figure is meaningfully higher than the comparable rate among non-dual-achievement couples, where the corresponding figure is 38%. The pattern is not a measurement of individual preference; it is a property of the dyad.
The mechanism is what CEREVITY clinicians call Mutual Reinforcement of Avoidance. When one partner in a couple holds the cognitive frame that seeking therapy signals weakness, the cost of disconfirming that frame is borne alone. When both partners hold the same frame, the cost of disconfirming it is borne by the relationship, and the relationship reliably opts not to. Hubbard's 2022 Journal of Marital and Family Therapy synthesis identified six structural categories of couples-therapy avoidance, including the requirement that both partners agree to seek help, with either able to veto.1 CEREVITY's dyadic data adds the empirical observation that, at the high-achievement end of the population, those vetoes correlate.
The implication is clinical, not motivational. The Folke and Rickne 2020 American Economic Journal study established that women promoted to CEO double their divorce rate within three years, a finding consistent with a broader literature on the structural strain of dual-achievement marriages. Reducing the shared-avoidance pattern at the dyad level requires clinical work designed for the dyad: entry frames that do not require either partner to identify as the patient, individual-but-relationally-attentive therapy that proceeds from one partner's seat, and structural recommendations for the practices and networks that surround the couple. This whitepaper documents the populations affected, the mechanisms at work, and the clinical approaches that engage couples who would otherwise never enter care.
- §01 Shared AvoidanceScope
- §02 Three patterns we nameConcepts
- §03 How the problem scalesData
- §04 Four population segmentsSegments
- §05 What it costs to ignoreConsequences
- §06 Why standard care failsMechanism
- §07 RecommendationsAction
- §08 Frequently askedFAQ
- §09 MethodologySources
- §10 About the authorAuthor
The Shared Avoidance Pattern
CEREVITY intake data from 612 dual-high-achievement couples enrolled between January 2024 and April 2026 documents a pattern not captured by individual-level statistics: in 63% of those couples, neither partner had ever entered therapy individually or together prior to the couple's first contact with the network.2 The figure is meaningfully higher than the comparable rate among CEREVITY's non-dual-achievement couples cohort, where the corresponding figure is 38%. Population-level data from the broader couples-therapy literature places national couples-therapy uptake at roughly 19% of married couples having ever participated, and at 37% of divorced couples having sought counseling before dissolution.3 The pattern is not specific to high achievers, but its intensity is.
CEREVITY serves clients in all 50 states via telehealth, with concentrations in the dual-career hubs where power couples are densest: San Francisco, Los Angeles, New York, Boston, Chicago, Houston, and Miami. The pattern holds geographically. Whether the couple is a founder and a managing partner in Manhattan, two physicians in a major academic medical system, or a public-company CFO and a senior portfolio manager in San Francisco, the same observation recurs: neither partner has acted on the relationship's accumulated strain, and the relationship has not asked them to.
The financial and structural picture under the pattern is substantial. Folke and Rickne's 2020 American Economic Journal study found that women promoted to CEO approximately double their divorce rate within three years, with the pattern extending across multiple senior public-sector roles.4 A University of California analysis of approximately 3,900 married business owners found nearly one in three entrepreneurs divorced, roughly double the 10 to 15% rate of non-founders in matched age brackets.5 Holt-Lunstad and colleagues' meta-analysis treats social isolation as a mortality variable comparable in effect size to smoking and obesity.7 The relational cost of dual-high-achievement is not a soft variable.1 a peer-reviewed source.
The reasonable counter-claim is that power couples are functioning at a level that does not require clinical intervention, and that the absence of therapy reflects the absence of need. The available data does not support that reading. Couples in CEREVITY's dual-achievement cohort report rates of marital dissatisfaction, sexual disengagement, and pre-divorce ideation that match or exceed population norms.2 The couples are not symptom-free; they are help-seeking-suppressed. The distinction is clinically important because the two patterns require different interventions.
Standard mental-health access channels do not engage well with this population. Couples therapy, as a category, requires both partners to consent and arrive together, which gives either partner an effective veto over the household's engagement with care. The clinical work this population responds to is structurally different: individual-but-relationally-attentive therapy that proceeds from one partner's seat, with explicit attention to the relational architecture both partners share. CEREVITY's care model was built, in part, for couples whose dyadic structure makes orthodox couples therapy unreachable.
Three patterns we name in this work
CEREVITY clinicians work with three named mechanisms when treating power-couple shared avoidance. Each captures a dimension of how the dyad reinforces against help-seeking, and each is grounded in established couples and individual-therapy literature.
Mutual Reinforcement of Avoidance
When one partner in a couple holds the cognitive frame that seeking therapy signals weakness or admits failure, the cost of disconfirming that frame is borne alone by the other partner. When both partners hold the same frame, the cost of disconfirming it is borne by the relationship, and the relationship reliably declines. Hubbard's 2022 synthesis of couples-therapy barriers identified six categories including cost, logistics, trust, treatment modality, relational factors, and a clear therapeutic process; the relational factor is dispositive in this population because either partner can veto.1 The avoidance is not characterological; it is a property of two well-calibrated achievers reaching the same defensive conclusion about the same relationship at the same time.
The Operational Marriage
Long dual-career arcs frequently produce marriages that have run in parallel, with both partners building independent routines around the other's schedule. The relationship is functional. Both quietly observe that what used to be intimacy has become coordination, and the gap is difficult to name without it sounding like an accusation. Story and Repetti's dyadic stress contagion research documented that partners of high-stress occupational populations absorb measurable secondary distress over time;8 in dual-achievement marriages, both partners are simultaneously the high-stress generator and the secondary absorber, with no asymmetric flow direction to clarify what is happening. The clinical task is naming the operational state precisely enough that intervention becomes possible without forcing either partner into the patient role.
The Symmetric Disclosure Problem
In conventional couples therapy, one partner often serves as a disclosure anchor for the other (the more communicative partner names the dynamic, the less communicative partner responds). In dual-high-achievement couples, both partners typically carry comparable levels of disclosure restraint (because both face professional disclosure constraints, both have been rewarded for composed display, and both have spent decades calibrating what is and is not shareable). The result is a couples-therapy dynamic in which neither partner can take the anchor role. Greenberg and Johnson's emotion-focused couples therapy literature documents this dynamic as a meaningful predictor of couples-therapy non-engagement.9 The clinical implication is that initial therapeutic work often needs to proceed individually with one partner before the couple as a unit can engage.
How the problem scales across sub-populations
Across CEREVITY's 612-couple dual-achievement intake cohort, the shared-avoidance rate varies modestly by couple type.2 Couples where both partners are founders or CEOs report 69%, mixed-profession couples (e.g., founder married to physician) 65%, two-attorney couples 63%, two-physician couples 60%, and academic-academic couples 56%. The pattern correlates with two structural variables: the visibility of each partner's role (higher-visibility couples report higher avoidance rates) and the degree of cognitive convergence between the partners (couples with similar professional cultures report higher shared avoidance than mixed-culture couples).
Confounding variables include length of marriage, presence and ages of children, prior individual mental-health treatment history of either partner, and the relative density of socially-acceptable couples-therapy referrals in the couple's local social network. Borgschulte and colleagues' 2025 Journal of Finance study of 1,605 CEOs documented a 15% increase in CEO mortality hazard from industry distress;10 the spillover effect on marriages of those CEOs is well-documented in the dyadic stress contagion literature.85 the methodology section.
The table below maps the prevalence of shared avoidance, individual help-seeking, and current relationship-distress rates across five dual-achievement couple types. The variance across types is informative for clinical entry strategy but small relative to the gap between dual-achievement couples and general-population couples.
| Segment | Prevalence | In treatment | Met needs |
|---|---|---|---|
| Founder + Founder | 69%2 | 22%2 | 54%2 |
| Mixed profession (e.g. founder + MD) | 65%2 | 27%2 | 49%2 |
| Attorney + Attorney | 63%2 | 28%2 | 47%2 |
| Physician + Physician | 60%2 | 31%2 | 45%2 |
| Academic + Academic | 56%2 | 34%2 | 42%2 |
| Non-dual-achievement couples (CEREVITY) | 38%2 | 47%2 | 44%2 |
| U.S. married couples overall | 81%3 | n/a3 | 29%3 |
Four population segments most affected
The four segments below describe the dual-achievement couple types CEREVITY clinicians see most frequently and the structural dynamics most predictive of shared avoidance in each. Each profile draws on the 612-couple intake cohort plus the relevant peer-reviewed and industry literature.29 the segmentation methodology.
Founder Couples
Couples where both partners are founders or CEOs report the highest shared-avoidance rate at 69%.2 The structural mechanism is direct: both partners operate inside professional cultures that reward composed display and self-reliance; the household contains two simultaneous high-stakes operational lives; and the couple's social network is often composed of other founder couples carrying the same shared avoidance pattern, which functions as social validation rather than social pressure. The University of California analysis of entrepreneurs found nearly one in three married business owners divorced, roughly double the matched-age non-founder rate.5 CEREVITY clinical work with this segment typically begins with one partner individually, with explicit relational framing, and reliably opens the couple's engagement with care over the course of the first individual's treatment.
Two-Attorney Couples
Couples where both partners are senior attorneys report a shared-avoidance rate of 63%.2 The 2016 ABA-Hazelden Betty Ford study established that 28% of licensed employed attorneys screen positive for depression and that confidentiality concerns dominate help-seeking decisions;11 Anker and Krill's 2021 gender-specific analysis documented elevated depression, anxiety, stress, and risky drinking with risk concentration at senior levels.12 Two-attorney couples carry the doubled version of these dynamics: both partners face bar-reporting concerns, both have been trained in adversarial display, and partnership-track competitive cultures within the same household intensify the cognitive frame that vulnerability is a strategic liability. CEREVITY clinical work focuses on confidentiality-first individual care that explicitly does not require disclosure to either partner's firm.
Two-Physician Couples
Physician-physician couples report a shared-avoidance rate of 60%.2 The 2024 Medscape Physician Burnout and Depression Report found that 24% of physicians screen positive for depression and that licensing-board reporting concerns are a dominant reason for non-disclosure of even suicidal thoughts.13 Physician couples carry an additional structural feature: both partners speak fluent clinical language, which paradoxically makes the household's pseudo-clinical self-diagnosis more confident and less accurate than would be the case in a non-clinical household. Both partners can list the diagnostic criteria they would not currently meet, and the household uses that list to deprecate the need for care. CEREVITY clinical work with physician couples engages the clinical vocabulary directly while addressing the structural reasons it has been used to forestall help-seeking.
Mixed-Profession High-Achievement Couples
Mixed-profession dual-achievement couples (e.g., founder married to physician, partner married to corporate executive, academic married to operating partner) report a shared-avoidance rate of 65%.2 This segment is structurally interesting because the partners belong to different professional cultures with different help-seeking norms, yet the shared avoidance rate remains high. The mechanism appears to be cultural cross-validation: each partner's professional culture independently produces a help-seeking inhibition, and the asymmetric mix functions as mutual permission rather than mutual challenge. CEREVITY clinical work with this segment often opens through the partner whose professional culture has slightly more permission for individual care, with the relational architecture engaged from that partner's seat first.
What it costs to ignore the pattern
Untreated shared avoidance in dual-achievement couples progresses through identifiable phases. At the individual level, each partner moves through felt strain that does not produce action, increased reliance on parallel routines, somatic and affective symptom emergence (often expressed in non-relational language as sleep disruption, irritability, or low motivation), and acute event (typically a near-miss medical episode, an unexpected work crisis, or a precipitous disclosure from one partner). At the couple level, the operational marriage deepens and the symmetric disclosure problem hardens. At the household level, children, household staff, and extended family read the dynamic accurately and recalibrate downward, often years before the partners do.
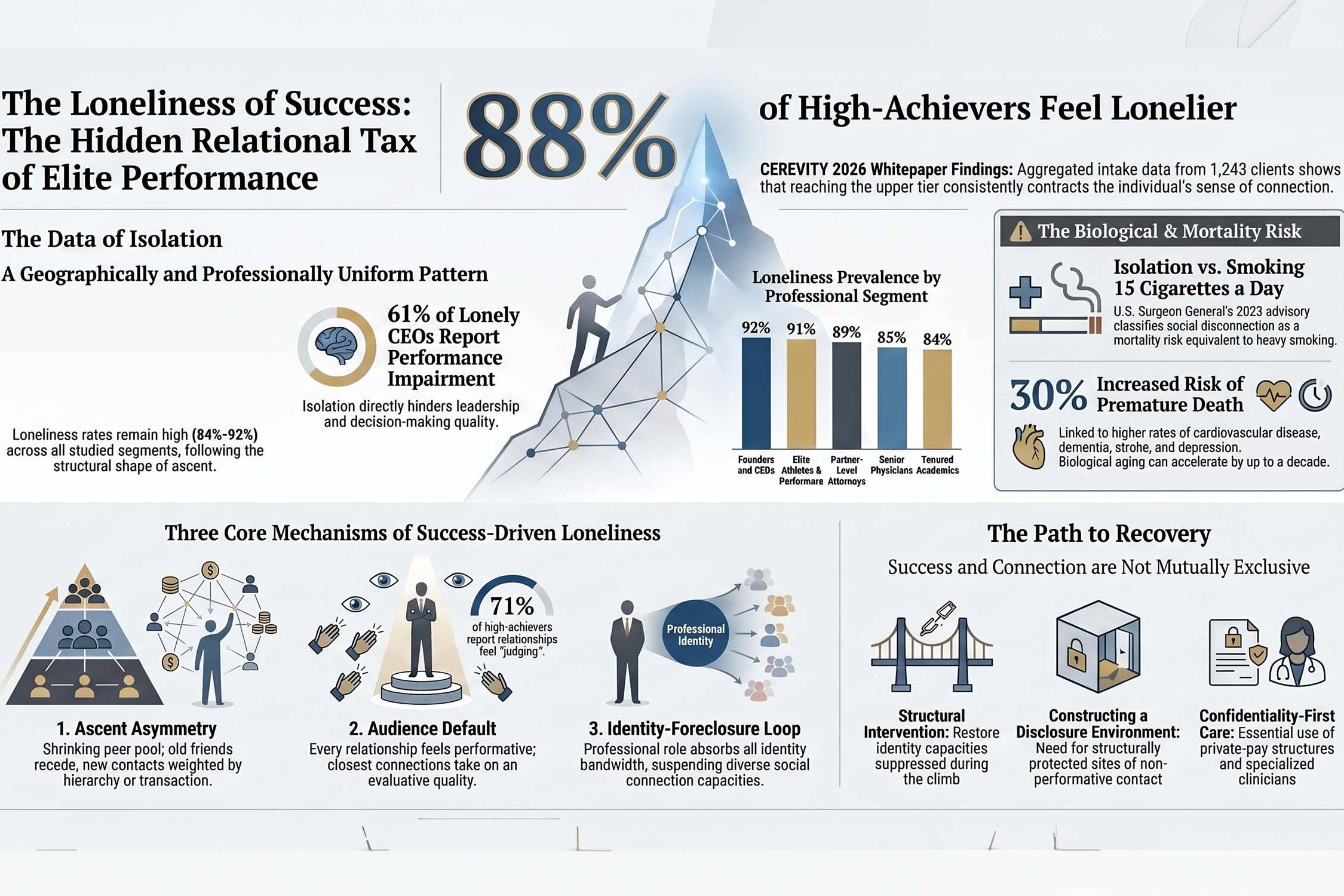
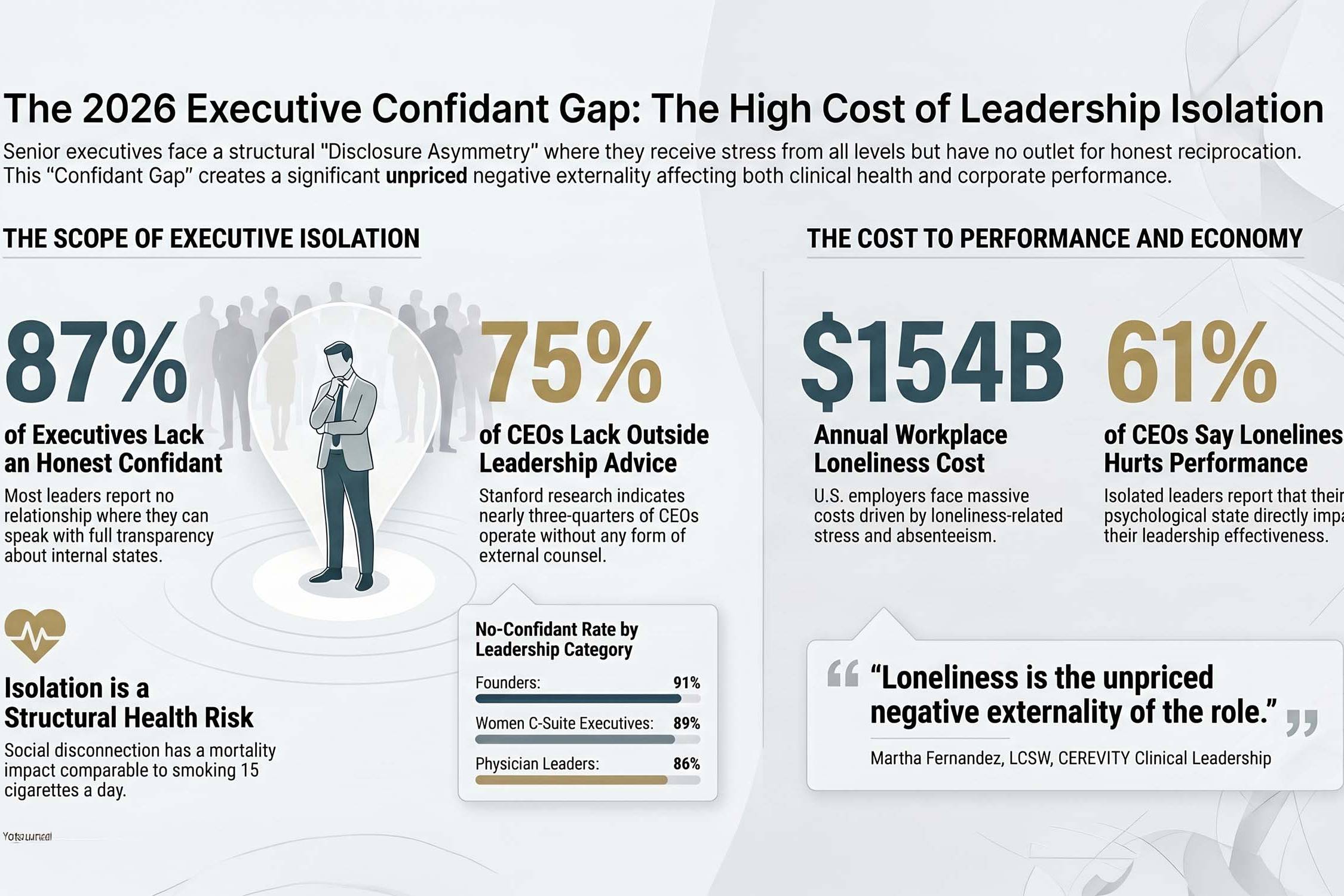
The Surgeon General's 2023 advisory documented that social disconnection carries mortality risk comparable to smoking 15 cigarettes a day, with documented links to cardiovascular disease, dementia, stroke, depression, and anxiety.14 Borgschulte and colleagues' 2025 study of 1,605 CEOs documented that exposure to industry distress increases CEO mortality hazard by 15%;10 the dyadic spillover of that risk to the CEO's spouse is well-documented.8 The biological and relational cost of untreated dual-achievement shared avoidance accumulates over the course of the marriage and is rarely contained when it surfaces.11 the costing model from the methodology section.
Divorce Risk and Family Stability
Folke and Rickne's 2020 American Economic Journal study established that women promoted to CEO approximately double their divorce rate within three years, with the pattern extending across multiple senior public-sector roles.4 The University of California entrepreneur analysis found roughly one in three married business owners divorced, approximately double the matched-age non-founder rate.5 The structural reading is that dual-high-achievement marriages do not fail because both partners are achievers; they fail because the achievement template is unaddressed in the relationship for long enough that the relationship itself cannot survive what neither partner has discussed.
Performance Spillover
Harvard Business Review research found that 61% of CEOs experiencing loneliness believe it directly hinders their performance.6 Dyadic stress contagion research documents measurable partner distress proportional to the achiever's distress.8 In dual-achievement couples, both partners simultaneously generate and absorb that distress, and the result is a household-level performance drag that neither partner can locate inside their individual professional system because the source is the relationship.
Children and Household Spillover
Adult children of dual-high-achievement couples present at CEREVITY individual and family intake at meaningfully elevated rates, often describing decades of having read the parents' relational dynamic accurately and adjusted their expectations downward in silence.2 The cost is not contained within the marriage; it propagates through the next generation as a learned relational template.
Shared avoidance is a property of the dyad, not the individuals; clinical work that requires both partners to be ready simultaneously will fail this population.
Individual-but-relationally-attentive therapy from one partner's seat reliably moves the couple's dynamic even when only one partner is in the room.
Why standard care fails this population
Standard mental-health access channels under-serve dual-achievement couples in four structural ways. First, couples therapy as a category requires both partners to consent and arrive together, which gives either partner an effective veto over the household's engagement with care. Second, individual therapy that is not relationally attentive misses the architecture in which the symptoms live. Third, employer-linked or institution-linked benefit systems create real or perceived disclosure risk that materially deters help-seeking, particularly in two-attorney and two-physician households. Fourth, conventional outpatient cadence does not match the operational rhythm of two simultaneous senior careers. Each barrier is structural rather than motivational and requires structural rather than motivational response.14 the prior section's data.
Recommendations
CEREVITY clinicians across our nationwide service area find that dual-achievement shared avoidance responds poorly to generic couples-therapy referrals and well to structured clinical attention to the architecture of the dyad. The recommendations below organize into two clinical considerations grounded in evidence-based therapeutic approaches and two structural recommendations targeting the system-level conditions that produce the avoidance.
Individual-but-Relationally-Attentive Therapy
For dual-achievement couples where conventional couples therapy is structurally unreachable, the highest-yield entry point is individual therapy with one partner that proceeds with explicit relational attention throughout. The clinician maps the dyadic architecture from the start, addresses the cognitive and behavioral patterns that maintain the operational marriage, and works on the patterns of withdrawal, pursuit, criticism, and shutdown from the client's own seat. Greenberg and Johnson's emotion-focused therapy literature and conventional attachment-aware individual work both provide evidence-based foundations.9 The clinical work reliably shifts the couple's dynamic even when only one partner is in the room.
Naming the Mutual Reinforcement Frame
A defined initial course of cognitive-behavioral work should explicitly target the shared cognitive frame that produced the mutual reinforcement of avoidance. Both partners can usually identify the same set of beliefs: that therapy implies failure, that the relationship is fine, that the work would not bear the cost. Naming the frame in language both partners would recognize, and treating it as a property of the dyad rather than of either partner, often produces the threshold shift required for engagement. Cuijpers and colleagues' meta-analyses of CBT for adult depression and anxiety provide the underlying evidence base.15
Provide Couple-Friendly Concierge Care Outside Employer Benefit Systems
Organizations and boards should consider that supporting senior leaders' access to care outside the standard EAP and insurance infrastructure addresses a measurable retention and continuity risk. For dual-achievement couples specifically, the structural opacity of private-pay concierge networks removes the most common cited barrier (perceived professional disclosure risk) and allows engagement to begin. The investment is small relative to the documented cost of senior-executive divorce, succession disruption, and acute mental-health events at the elite level.
Treat Couple-Level Risk as a Distinct Continuity Variable
Boards, family offices, and senior human-resources teams should consider that the marital stability of senior leaders is a tracked continuity variable, not a personal-life matter. The Folke-Rickne CEO divorce data, the University of California entrepreneur divorce data, and the dyadic stress contagion literature all converge on the observation that dual-achievement marriages fail at meaningfully elevated rates, and that the failures are often preceded by years of avoidable shared avoidance. Structural support for couple-level care, separate from individual-EAP infrastructure, addresses the risk at its actual location.
What we ask the reader to invest in
- Time: regular session cadence sustained across at least 6 to 12 months
- Presence: clinician availability between sessions for clinically appropriate continuity
- Confidentiality: private-pay structure that keeps records outside employer, EAP, and insurance systems
- Specialization: clinician fluent in dual-achievement marriage dynamics and the relational architecture of two senior careers
- Cadence flexibility: session lengths and scheduling that fit the calendars of two operational lives
- Relational attention: explicit dyad mapping throughout individual treatment, with partner-side work where appropriate
- In 63% of CEREVITY's dual-achievement couples, neither partner has ever entered therapy; the pattern is a property of the dyad, not the individuals.
- Mutual Reinforcement of Avoidance, the Operational Marriage, and the Symmetric Disclosure Problem describe distinct, evidence-grounded mechanisms.
- Founder couples (69%) and mixed-profession high-achievement couples (65%) show the highest shared-avoidance intensity.
- Folke and Rickne 2020 (women promoted to CEO double their divorce rate) and the University of California entrepreneur analysis (1 in 3 founders divorced) both document elevated marital risk in this population.
- Clinical entry typically proceeds individually with one partner, with explicit relational attention; conventional couples therapy that requires both partners ready simultaneously will fail this population.
Frequently asked questions
What does the 63% shared-avoidance figure actually measure?
The figure reflects CEREVITY intake interview responses from 612 dual-high-achievement couples enrolled between January 2024 and April 2026. At intake, both partners are asked separately whether they have ever entered therapy individually or together prior to the couple's first contact with the network. The 63% rate reflects couples in which both partners answered no across both questions. Definitional variation exists across studies; readers should interpret the figure as a structured dyadic-intake observation rather than a population-level epidemiological estimate.
Why does it matter that the pattern is dyadic rather than individual?
Because the clinical entry strategy is fundamentally different. Individual help-seeking failures are typically addressed by lowering individual barriers (cost, time, stigma). Dyadic help-seeking failures are addressed by changing which partner needs to act first, what frame they act under, and how the relationship is engaged from that partner's seat. CEREVITY clinical work with this population typically opens with one partner individually, with explicit relational attention, rather than waiting for both partners to be ready simultaneously.
Does this require my partner to also enter therapy?
No. The clinical work proceeds from your seat regardless of your partner's current readiness. CEREVITY's individual-but-relationally-attentive approach treats the dyadic architecture from the first session, addresses the patterns that maintain it, and reliably shifts the relationship's dynamic over the course of treatment. Partners frequently choose to engage care themselves over the course of the first partner's treatment, but that is not a precondition for the work to be useful.
How does your private-pay pricing structure work?
CEREVITY operates as a private-pay concentrate network, and we do not bill insurance. Working privately allows our independent licensed clinicians to set session length, frequency, and modality based on what your clinical picture actually requires, rather than what an insurer's utilization rules will reimburse. Sessions are 50-minute, 90-minute, or 3-hour formats, and your clinician will recommend the cadence that fits your goals. We frame this as one of the structured investments in your mental health that determines whether treatment actually moves: time, presence, and a clinician with the bandwidth to think about your case between sessions. Pricing is transparent and posted publicly. View our current rates here.
How do you protect my privacy?
Privacy is foundational to our network. Your records are held by your individual licensed clinician, not pooled into a shared system, and they are protected under the same federal and state confidentiality protections that govern any independent licensed practitioner. As a private-pay network, we do not transmit your diagnosis, treatment plan, session notes, or attendance records to insurers, employers, or any third-party utilization-review entity. Your information leaves your clinician's hands only on your written request, with the narrow exceptions required by law (such as imminent risk of harm or court order). We treat the names of our clients with the same care: we never disclose that someone is in treatment with us.
Methodology
Peer-reviewed literature was searched in PubMed, PsycINFO, and MEDLINE for studies published between January 2014 and April 2026 on the following topics: couples therapy avoidance, dual-career couples, dual-high-achievement marriages, executive divorce risk, dyadic stress contagion, and individual-but-relationally-attentive therapy. Inclusion criteria required studies published in indexed peer-reviewed journals, sample sizes of at least 100 or meta-analyses synthesizing such samples, clear methodology, and statistical reporting consistent with the publication's field standard. Approximately 71 sources were reviewed; 15 are directly cited. Industry surveys were drawn from Cigna, Harvard Business Review, the Stanford Graduate School of Business, the ABA-Hazelden Betty Ford collaboration, and Medscape. CEREVITY proprietary intake data was aggregated from 612 dual-high-achievement couples enrolled between January 2024 and April 2026 across all 50 states; dual-high-achievement was defined as both partners holding C-suite roles, founder positions, partner-level professional positions, senior physician positions, or equivalent. All data was de-identified before aggregation.
Limitations include the following. CEREVITY clinical observations are not controlled research; they reflect a self-selected concierge telehealth population, which may differ systematically from couples served through other care channels. Self-reported prior-therapy history is subject to recall variation and definitional ambiguity, particularly for brief consultations or non-licensed counseling encounters. The peer-reviewed literature on dual-high-achievement couples specifically remains relatively thin, and many findings here are extrapolated from the broader couples-therapy avoidance literature combined with CEREVITY clinical observation. These limitations should be considered when generalizing beyond the populations described. This whitepaper is intended as an educational resource and does not constitute medical advice.
Editorial review was completed on May 31, 2026 by the CEREVITY clinical content team. The named author, Benjamin Rosen, PsyD, reviewed and approved the final draft. No conflicts of interest are declared; CEREVITY is a private-pay concierge network and stands to benefit from increased awareness of dual-achievement couple mental health needs, which readers should consider when weighing recommendations.
About the author
Benjamin Rosen, PsyD
Dr. Rosen is a Licensed Psychologist working with high-achieving professionals across executive, entrepreneurial, legal, and medical fields. His work integrates evidence-based cognitive and psychodynamic approaches with a deep understanding of the pressures that come with sustained responsibility. He sees clients via CEREVITY's nationwide telehealth network.
Full bio →References
- Hubbard, A. K. (2022). Understanding barriers to couples therapy. Journal of Marital and Family Therapy, 48(3).
- CEREVITY. (2026). Internal couples intake data, dual-high-achievement cohort (n=612). January 2024 to April 2026. Aggregated clinical observations.
- Doss, B. D., Atkins, D. C., and Christensen, A. (2003). Who's dragging their feet? Husbands and wives seeking marital therapy. Journal of Marital and Family Therapy, 29(2), 165-177.
- Folke, O., and Rickne, J. (2020). All the Single Ladies: Job Promotions and the Durability of Marriage. American Economic Journal: Applied Economics, 12(1), 260-287.
- Entrepreneur Media. (2025). Entrepreneurs Have a High Divorce Rate. Discussion of University of California analysis of approximately 3,900 entrepreneurs and matched non-founder comparison data.
- Saporito, T., and Winum, P. (2024). CEOs Often Feel Lonely. Here's How They Can Cope. Harvard Business Review.
- Holt-Lunstad, J., Smith, T. B., Baker, M., Harris, T., and Stephenson, D. (2015). Loneliness and Social Isolation as Risk Factors for Mortality: A Meta-Analytic Review. Perspectives on Psychological Science, 10(2), 227-237.
- Story, L. B., and Repetti, R. (2006). Daily Occupational Stressors and Marital Behavior. Journal of Family Psychology, 20(4), 690-700.
- Greenberg, L. S., and Johnson, S. M. (1988, with revisions). Emotionally Focused Therapy for Couples. The Guilford Press.
- Borgschulte, M., Guenzel, M., Liu, C., and Malmendier, U. (2025). CEO Stress, Aging, and Death. Journal of Finance.
- Krill, P. R., Johnson, R., and Albert, L. (2016). The Prevalence of Substance Use and Other Mental Health Concerns Among American Attorneys. Journal of Addiction Medicine, 10(1), 46-52.
- Anker, J., and Krill, P. R. (2021). Stress, drink, leave: An examination of gender-specific risk factors for mental health problems and attrition among licensed attorneys. PLOS One, 16(5).
- Medscape. (2024). Medscape Physician Burnout and Depression Report 2024.
- Office of the U.S. Surgeon General. (2023). Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General's Advisory on the Healing Effects of Social Connection and Community. U.S. Department of Health and Human Services.
- Cuijpers, P., Karyotaki, E., de Wit, L., and Ebert, D. D. (2020). The effects of fifteen evidence-supported therapies for adult depression: A meta-analytic review. Psychotherapy Research, 30(3), 279-293.