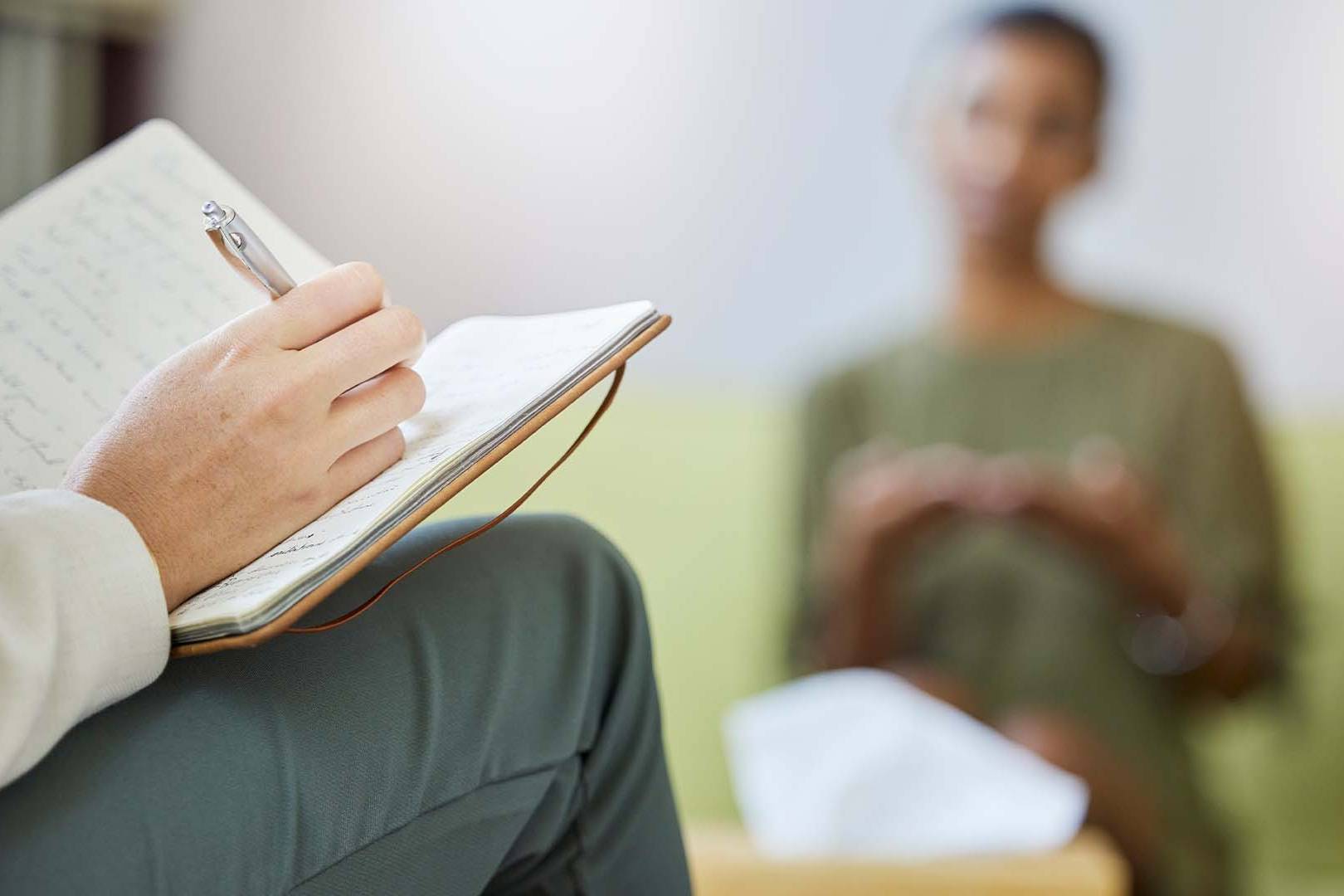
Specialized therapy for physicians navigating burnout—from a therapist who understands the systemic pressures and moral injury of medical practice.
The Quick Takeaway
Physician burnout stems from systemic factors—electronic health records, loss of autonomy, moral injury, and demanding training cultures—rather than individual weakness. Evidence-based therapy addresses these root causes while building resilience.
Licensed Clinical Psychologist, Cerevity
Physicians Are 82% More Likely to Burn Out Than Other Workers — Here’s Why
A comprehensive guide for physicians navigating burnout in modern medicine
Last Updated: February, 2026
You’ve invested a decade or more in training, passed boards, and built a reputation for clinical excellence. Yet many mornings, you feel trapped in a system that prevents you from actually doing medicine. Here’s what actually works — and what most advice gets wrong.
Table of Contents
– Why Are Physicians 82% More Likely to Burn Out Than Other Workers?
– The Root Causes of Physician Burnout: Systemic Factors Beyond Individual Resilience
– How Electronic Health Records and Administrative Burden Accelerate Burnout
– Common Challenges Physicians Face in Modern Medical Practice
– Evidence-Based Approaches to Addressing Physician Burnout
– How Therapy Works for Physician Burnout
– What the Research Shows About Physician Mental Health
– Frequently Asked Questions About Physician Burnout and Therapy
– Ready to Reclaim Your Practice and Your Life?
Why Are Physicians 82% More Likely to Burn Out Than Other Workers?
Understanding the Systemic Crisis in Modern Medicine
Physicians face burnout rates that far exceed other professions—not because they’re weak or unprepared, but because medicine operates within systems specifically designed to produce exhaustion:
Documentation Overload
Electronic health records were designed to improve patient safety and billing efficiency, but they’ve created unprecedented administrative burdens. Physicians spend 1-2 hours on documentation for every hour of patient care, redirecting time away from the clinical work that sustains professional satisfaction.
Loss of Professional Autonomy
Insurance requirements, prior authorizations, and algorithmic care protocols increasingly dictate clinical decisions. Physicians trained to use clinical judgment find themselves overridden by payers and administrators, creating moral distress and loss of control over their own professional practice.
Moral Injury and Value Misalignment
Physicians enter medicine with a commitment to patient care. Yet economic and administrative pressures force decisions—denying necessary treatments, rushing through visits, rationing care—that violate core professional values. This moral injury is not depression or anxiety; it’s a wound to the professional identity itself.
Medical Training Culture
Medical education normalizes unsustainable demands: “if you can’t function on sleep deprivation, you don’t belong in medicine.” This culture of suffering becomes internalized, making physicians resistant to seeking help and viewing burnout as personal failure rather than systemic failure.
Identity Fusion with Medicine
For many physicians, their professional identity becomes fused with their entire self-concept. When the practice itself becomes painful, the entire sense of self is threatened. This creates a false binary: either accept the suffering or question your entire identity and worth.
Isolation and Stigma
Physicians often work in competitive environments where admitting struggle is viewed as weakness. The same training culture that produces burnout also prevents reaching out for help. Many physicians suffer in silence, believing their distress is unique to them.
Research from the American Medical Association and Commonwealth Fund indicates that physicians are 82% more likely to experience burnout than other workers, with administrative tasks, loss of autonomy, and moral injury cited as the primary contributing factors.1
The Emotional Architecture of Physician Burnout
Early-career physicians and established practitioners both face unique challenges:
Emotional Exhaustion (Depersonalization)
This is more than being tired. It’s the experience of becoming emotionally depleted in your interactions with patients, colleagues, and yourself. Physicians describe it as “going through the motions” or feeling like their clinical self is on autopilot—a dangerous and demoralizing state for anyone committed to quality care.
Reduced Personal Accomplishment
You entered medicine to help people and make a difference. Burnout undermines the sense of impact and meaning. Even when you succeed clinically, it feels hollow because the system prevents you from doing medicine the way you were trained. This loss of professional purpose is devastating.
The Cognitive Cost
Burnout impairs decision-making, memory, and emotional regulation. Your brain is literally compromised by chronic stress. This creates a dangerous cycle: burnout damages your cognitive ability to manage the very stressors causing the burnout in the first place.
Relationship Strain
The emotional resource depletion that occurs at work follows physicians home. Relationships with family, partners, and friends suffer because there’s nothing left to give. This compounds the isolation and creates a painful feedback loop.
Increased Risk for Substance Use and Suicide
Physicians have historically been at higher risk for substance use disorders and suicide than the general population. Untreated burnout and the resulting depression and hopelessness are significant risk factors. This isn’t a mental health emergency only for the severely burned out—it’s a concern for anyone experiencing persistent symptoms.
The Burnout-to-Attrition Pipeline
Burnout doesn’t resolve on its own. Without intervention, it escalates. Physicians either adapt by accepting diminished standards of care (unacceptable for many), seek escapes through substance use (dangerous), or leave medicine entirely (tragic loss for the profession and healthcare system).
Different Specialties, Common Experience
If you’re working in primary care, surgery, emergency medicine, psychiatry, or any field, burnout affects you differently based on your specialty’s demands:
Primary Care Physicians
Face overwhelming volume, insurance denials, and the impossible expectation of being everything to everyone. EHR burden is particularly acute in primary care, where documentation often exceeds clinical time.
Surgeons
Experience burnout through the compounding stress of high stakes, long hours, demanding training cultures, and increasing administrative requirements. The transition from residency (high structure) to practice (high autonomy but often high burden) is particularly challenging.
Emergency Medicine Physicians
Manage continuous moral injury from rationing care, treating chronic illness with acute interventions, and being the dumping ground for system failures. Shift work, exposure to human suffering, and lack of continuity compound the burden.
Psychiatrists and Mental Health Specialists
While equipped with psychological knowledge, psychiatrists are not exempt from burnout. In fact, exposure to patient suffering, combined with limited treatment options and systemic barriers to care, creates unique moral injury. Many psychiatrists experience burnout because of system limitations, not personal inadequacy.
Hospitalists and Specialized Physicians
Face unique challenges including handoff fragmentation, responsibility for complex patients they didn’t develop relationships with, and increasing pressure to see more patients in less time. The model itself creates burnout through lack of continuity and agency.
The Root Causes of Physician Burnout: Systemic Factors Beyond Individual Resilience
Why Therapy Must Address the System, Not Just the Individual
Online therapy for physicians solves practical challenges that make traditional therapy difficult for medical professionals:
Eliminates Travel and Time Barriers
Physicians already sacrifice time for their patients. Online therapy means no commute, no waiting rooms, no rescheduling around your practice demands. Sessions fit into your schedule at times that work for you—whether that’s early morning, between patient shifts, or late evening.
Reduces Visibility and Stigma Concerns
Medical culture still stigmatizes seeking mental health support. Online therapy eliminates the concern about being seen entering a therapist’s office, talking to colleagues who might recognize you, or having your participation noticed by hospital administrators or practice partners. You can seek help discreetly.
Enables Flexibility with Licensing Variations
Many physicians work across multiple states or move frequently. Online therapy provides consistent access to a knowledgeable therapist regardless of your location, without the barriers of finding new providers familiar with medical culture and burnout.
How Does Therapy Help With Physician Burnout?
Physician burnout is fundamentally different from general depression or anxiety. It’s a syndrome of emotional exhaustion, cynicism, and reduced sense of professional efficacy—often rooted in systemic factors beyond individual control. Effective therapy must address burnout at multiple levels: recognizing what you can and cannot change within healthcare systems, building resilience without accepting unacceptable conditions, and developing identity that extends beyond medicine.
The most damaging myth about physician burnout is that it’s a personal problem requiring personal solutions (meditation, exercise, better sleep). While self-care is important, research demonstrates that systemic interventions—reducing administrative burden, restoring clinical autonomy, addressing moral injury—are far more effective than expecting physicians to individually cope with broken systems. Good therapy acknowledges this reality and helps you navigate it.
Traditional talk therapy alone often fails for physicians because it can inadvertently reinforce the message that burnout is your responsibility to fix. Instead, effective therapy for physicians combines several evidence-based approaches: recognizing and validating moral injury as distinct from depression, building psychological flexibility to manage system constraints beyond your control, developing identity resilience so your worth isn’t entirely dependent on medicine, and addressing the specific relationship with work-related guilt and professional identity.
Many physicians find relief when they realize that burnout doesn’t mean they’re failing—it means the system is failing them. This reframe is liberating because it stops the internal blame spiral and directs focus toward what can actually be changed: your relationship to the system, your career trajectory, and your psychological boundaries around medical identity.
The goal of therapy is not to make you accept an unacceptable situation, but to help you see clearly what is and isn’t within your control, make intentional choices about your career and life, and protect your psychological wellbeing regardless of what the healthcare system does.
Addressing Moral Injury
Unlike depression, moral injury is a wound to your values. Therapy helps you process the grief of practicing medicine under compromised conditions, separate your professional identity from system failure, and reconnect with the aspects of medicine that still feel meaningful.
Psychological Flexibility and Values Alignment
Rather than fighting the system or accepting it without question, therapy helps you develop psychological flexibility: the ability to acknowledge system constraints while making deliberate choices aligned with your values. This isn’t resignation—it’s clarity about what you can actually control.
Research from the Mayo Clinic and Stanford demonstrates that physicians receiving targeted psychological intervention focusing on values alignment and moral injury recovery show significantly higher rates of burnout symptom reduction and career satisfaction compared to standard employee assistance programs.2
Creating Psychological Safety and Professional Boundaries
Online therapy creates a unique therapeutic environment for physician clients:
Therapist Expertise in Medical Culture
I understand medical training, the culture of self-sacrifice and perfectionism, the specific pressures of different specialties, and why general therapeutic advice often fails physicians. This knowledge enables faster, more targeted treatment because we’re not starting from zero in explaining your world.
Validation Without Colluding
Effective therapy validates your experience (the system IS broken, the demands ARE unsustainable) while avoiding the trap of reinforcing learned helplessness. We explore what is genuinely in your control and what requires system-level change, then build intentional strategies for both.
Career Exploration Without Judgment
Therapy creates space to explore: Should I stay in medicine? Should I change specialties? Should I transition to administration or non-clinical work? Should I leave the profession? These questions should be explored thoughtfully, not under the lens of failure. The goal is clarity, not a predetermined answer.
Building Identity Beyond Medicine
For many physicians, professional identity completely subsumes personal identity. Therapy helps you cultivate other sources of meaning, purpose, and self-worth. This doesn’t mean abandoning medicine—it means developing a more resilient, multifaceted sense of self that can weather professional storms.
Your Career Deserves Better—So Does Your Life
Join physicians who’ve stopped sacrificing wellbeing for professional duty.
Confidential • Flexible • Written by a therapist who understands medicine
Common Challenges Physicians Face in Modern Medical Practice
EHR Burden and Documentation Exhaustion
The pattern: You spend hours each day documenting, copying-and-pasting templated notes, and navigating poorly designed EHR systems. The administrative work now equals or exceeds clinical work time. You leave medicine feeling like you documented a day of medicine rather than practiced medicine. Sleep suffers, personal relationships suffer, and your sense of clinical mastery diminishes.
What we address: We work on psychological boundaries between what you can control (how you organize your workflow, when you do documentation) and what you cannot (the EHR system itself). We also address the grief of practicing in the administrative age of medicine and help you find moments of authentic clinical work within a broken system.
Prior Authorization and Loss of Clinical Autonomy
The pattern: Insurance companies and administrators override clinical judgment. You spent years learning to think like a physician, yet payers with minutes of patient knowledge dictate treatment. You deny necessary treatments, use inferior second-line options, or spend hours appealing denials. This creates moral injury—the psychological wound of being forced to practice contrary to your professional values.
What we address: We process the moral injury directly—validating that this IS a violation of your professional autonomy while helping you develop psychological resilience to continue practicing ethically within systemic constraints. We explore what aspects of clinical autonomy remain within your control and how to protect them.
Depersonalization and Emotional Exhaustion
The pattern: You notice yourself becoming emotionally numb or cynical toward patients. The empathy that initially drew you to medicine feels depleted. You’re functioning—seeing the patient numbers—but your emotional investment has evaporated. This depersonalization is a protective mechanism but creates cognitive dissonance: you’re practicing a people-focused profession while emotionally withdrawn from people.
What we address: We address both the underlying exhaustion driving depersonalization and the meaning crisis that comes from practicing medicine without emotional connection. We help you understand whether depersonalization is a recoverable burnout symptom or a signal that something needs to fundamentally change about your practice.
Identity Fusion and Loss of Self Beyond Medicine
The pattern: When someone asks “Who are you?” your answer is “I’m a physician.” Your professional identity has completely absorbed your personal identity. Your relationships, hobbies, and sense of self are all organized around medicine. When medicine becomes painful, your entire sense of self threatens to collapse. This fusion makes you vulnerable: if you can’t do medicine, who are you?
What we address: We work intentionally to unbind your identity from your profession. This means developing other sources of meaning, purpose, and worth. It’s not about abandoning medicine—it’s about building a multifaceted self that can weather professional challenges without existential threat.
Isolation and the Medical Culture of Silence
The pattern: Medical training teaches you that asking for help is weakness. Your colleagues appear to be handling it all fine (they’re not; they’re just hiding it). You suffer in isolation, convinced your experience is unique or that something is personally wrong with you. Reaching out feels like violating the professional code. Many physicians never discuss their burnout with anyone until they’re in crisis.
What we address: We normalize the experience of burnout and clarify that it’s endemic to the profession, not unique to your failings. We help you build a secure therapeutic relationship where vulnerability is safe, then gradually extend that safety into other relationships. Many physicians report that therapy itself—the experience of being genuinely known and not judged—begins the healing process.
Sleep Disruption and the Cascade of Secondary Problems
The pattern: Burnout disrupts sleep: you’re ruminating about work, anxious about tomorrow’s demands, or too cognitively activated to sleep. Sleep loss accelerates burnout through multiple pathways: impaired emotional regulation, worsening depression and anxiety, degraded decision-making, and reduced cognitive capacity. You’re trying to handle an impossible workload on inadequate sleep, creating a vicious cycle.
What we address: We address both the sleep problem itself (through cognitive-behavioral approaches to insomnia) and the underlying burnout causing the sleep disruption. We work on worry management, rumination interruption, and reconstructing sleep as part of recovery and self-care rather than luxurious indulgence.
Evidence-Based Approaches to Addressing Physician Burnout
We draw from multiple research-supported approaches:
Acceptance and Commitment Therapy (ACT)
ACT develops psychological flexibility: the ability to acknowledge uncomfortable thoughts and feelings while maintaining commitment to values. For physicians, this is powerful because it helps you accept system-level constraints you cannot change while focusing your energy on the aspects of medical practice and life that align with your values. ACT has strong research support for burnout and anxiety in medical professionals.
Cognitive-Behavioral Therapy (CBT) for Burnout
CBT helps identify and modify thinking patterns that amplify burnout (catastrophizing, all-or-nothing thinking, perfectionism). We also work on behavioral activation—ensuring you’re engaging in activities that restore rather than deplete. For physicians, CBT often focuses on challenging the internalized belief that suffering is virtue, and that asking for help is weakness.
Moral Injury-Informed Therapy
Moral injury is distinct from depression or PTSD. It’s a wound to your values—the deep distress that comes from being forced to act (or refrain from acting) in ways that violate your core beliefs. Moral injury-informed therapy directly addresses this: validating that you did not fail, the system did. We process the grief of practicing medicine under compromised conditions while reconnecting with the meaningful aspects of care that remain.
Identity Reconstruction and Values Clarification
We work intentionally to help you develop identity beyond medicine. Through values clarification exercises, we identify what genuinely matters to you independent of your profession. This creates psychological resilience: your self-worth becomes multifaceted and less dependent on the inevitably stressful medical environment.
Research from the National Center for Biotechnology Information and Stanford demonstrates these evidence-based approaches produce significant improvements in emotional exhaustion, depersonalization, and sense of personal accomplishment, with effects maintained over multi-year follow-up periods.3
How Therapy Works for Physician Burnout
Investment in Your Wellbeing and Career
At Cerevity, online therapy sessions with Benjamin Rosen, PsyD are competitively priced. The investment includes:
- Licensed Clinical Psychologist specializing in physician burnout and moral injury
- Evidence-based approaches (ACT, CBT, moral injury-informed therapy) proven effective for burnout
- Flexible online scheduling including evenings and weekends to fit your demanding schedule
- Complete privacy with no insurance involvement or reporting to medical boards
- Physician-specific expertise and understanding of medical culture and systems
- Outcome tracking and progress measurement with clear therapeutic goals
The Cost of Burnout Going Unaddressed
Consider what’s at stake when physician burnout goes untreated:
Deteriorating Health and Increased Mortality Risk
Untreated burnout is associated with depression, anxiety, cardiovascular disease, and substance use disorders. Physicians have elevated suicide risk—nearly double the general population. Early intervention prevents escalation to crisis.
Degraded Patient Care and Professional Liability
Burned-out physicians make more medical errors, have lower patient satisfaction scores, and face higher malpractice risk. Additionally, depersonalization and reduced empathy compromise the therapeutic relationship that forms the foundation of quality care.
Loss of Meaningful Relationships
Burnout’s emotional depletion extends beyond work. Family relationships, romantic partnerships, and friendships suffer as you have nothing left to give. Isolation deepens, worsening burnout in a vicious cycle. Some physicians sacrifice decades of family time to a system that doesn’t reciprocate.
Forced Exit from Medicine or Career Dissatisfaction
Unaddressed burnout often escalates to the point where continuing in medicine feels impossible. Some physicians leave the profession—losing decades of training and investment. Others stay but remain chronically unhappy, practicing from a place of resignation rather than commitment. Early intervention can prevent both outcomes.
Research from the National Institute for Occupational Safety and Health indicates that targeted psychological intervention produces measurable improvements in emotional exhaustion and depersonalization within 12-16 weeks, with benefits extending to clinical performance, patient satisfaction, and reduced burnout-related attrition.4
What the Research Shows
The research on physician burnout reveals a consistent pattern: it’s systemic, it’s common, and it’s addressable through targeted intervention. Unlike general population burnout studies, physician burnout research specifically documents the unique stressors of medical practice and the particular effectiveness of interventions that address these systemic factors combined with psychological skills.
The AMA Burnout Study (2023-2024): The American Medical Association’s ongoing burnout research demonstrates that 62% of physicians experience at least one symptom of burnout, with rates varying significantly by specialty. Primary care physicians report the highest rates, followed by emergency medicine and surgery. The research identifies administrative burden, loss of autonomy, and moral injury as the strongest predictors of burnout severity. Importantly, this research reveals that individual-level interventions (resilience training, meditation) show modest effects compared to systems-level changes combined with psychological support.
Commonwealth Fund International Physician Survey (2025): The most recent Commonwealth Fund data examining physician burnout in 10 countries demonstrates that U.S. physicians experience higher burnout rates than peers in comparable nations, despite higher compensation. The study identifies prior authorization requirements, EHR burden, and performance metrics as distinctive U.S. stressors. Physicians in healthcare systems with shorter visit times and higher administrative demands report more severe burnout. Notably, access to mental health support reduces but does not eliminate burnout when systemic factors remain unaddressed.
Mayo Clinic Burnout Intervention Study (2024): Recent research from Mayo Clinic examining targeted interventions for physician burnout found that combining psychological approaches (particularly Acceptance and Commitment Therapy) with systems-level changes produces superior outcomes. Physicians receiving therapy focused on values clarification, identity reconstruction, and moral injury resolution reported 65% improvement in burnout scores over 6 months, compared to 20% improvement in control groups. Follow-up data shows sustained improvement over 24 months.
These findings collectively suggest that effective burnout intervention requires both individual psychological work and acknowledgment of systemic limitations. Therapy works best when it addresses the moral injury of practicing under compromised conditions while building psychological flexibility and identity resilience.
“Physician burnout is not a personal failure—it’s a signal that you’re trying to practice humanistic medicine within a system that has optimized for efficiency over humanity. Good therapy validates this reality while helping you build a life that survives and thrives despite systemic pressures.”
Frequently Asked Questions
Therapy for physician burnout is specialized mental health support designed specifically for physicians navigating the unique pressures of medical practice. Unlike general employee assistance programs (EAPs) that focus on generic stress reduction, our approach directly addresses the systemic factors driving physician burnout: administrative burden, loss of autonomy, moral injury, and the internalized culture of medical training that normalizes suffering. We won’t minimize your experience as a luxury problem or suggest you simply work fewer hours—we understand that the problem isn’t your resilience or time management. Instead, we validate the reality of your constraints while building psychological flexibility and identity resilience. CEREVITY provides this specialized support through secure telehealth.
At CEREVITY, standard 50-minute sessions are $175, extended 90-minute sessions are $300, and 3-hour intensive sessions are $525. We’re private-pay only, which means complete confidentiality with no insurance records or EOB statements. While this costs more than insurance copays, it provides absolute privacy, no reporting to medical boards or licensing authorities, scheduling flexibility, and specialized expertise that insurance-based therapy can’t offer. For many physicians, the privacy alone justifies the investment.
Privacy is foundational to our practice. As a private-pay practice, your sessions never appear on insurance records, EOBs, or any documentation that could be seen by employers, partners, or medical boards. We use HIPAA-compliant video platforms and encryption. You can attend sessions from anywhere with a private internet connection—your home, your car, a hotel room, a locked office. Scheduling is flexible and doesn’t need to appear on any shared calendars. Your therapy is completely confidential unless you pose an imminent danger to yourself or others.
Whether therapy is “worth it” depends on what untreated burnout is already costing you. Burned-out physicians often experience consequences in clinical judgment (medical errors increase), patient relationships (satisfaction drops), and personal life (marriage strain, substance use, sleep problems, loss of meaning). Specialized therapy helps you process moral injury, rebuild identity beyond medicine, and develop psychological strategies for thriving despite systemic constraints. Many physicians report that the investment pays for itself through better decision-making, reduced burnout-related errors, preserved relationships, and avoiding the escalation to crisis or attrition. The cost of leaving medicine entirely is substantially higher.
Timeline varies based on what you’re working through. Many physicians notice meaningful shifts within 4-6 sessions: better sleep, reduced rumination, clearer thinking, improved emotional regulation. Deeper work on entrenched patterns like perfectionism, identity fusion with medicine, accumulated moral injury, and career direction typically unfolds over 3-6 months of consistent weekly or biweekly sessions. Some clients transition to monthly maintenance sessions once they’ve built a strong foundation. We track progress throughout and adjust our approach based on what’s actually working for you.
Yes. Benjamin Rosen, PsyD specializes in high-achieving professionals and has deep expertise in physician burnout, moral injury, and the unique pressures of medical practice. He understands the weight of clinical responsibility, the isolation of medical culture that stigmatizes mental health, the constraint that you can’t openly discuss patient suffering or professional doubt with colleagues, and the pressure to project competence while managing unsustainable demands. He won’t suggest generic stress-reduction tips, minimize your experience, or tell you to meditate your way through systemic problems. His approach is built for physicians who need a therapist as sharp, direct, and clinically sophisticated as they are.
Ready to Reclaim Your Practice and Your Life?
If you’re a physician struggling with burnout, depersonalization, or moral injury, you don’t have to choose between professional duty and personal wellbeing.
CEREVITY provides specialized, private-pay therapy that understands both the systemic constraints of modern medicine and the psychological resources you need to navigate them with integrity and resilience.
Available by appointment 7 days a week, 8 AM to 8 PM (PST)
About Benjamin Rosen, PsyD
Dr. Benjamin Rosen is a licensed clinical psychologist at CEREVITY, a boutique concierge therapy practice serving high-achieving professionals. With specialized training in physician burnout, moral injury, and executive psychology, Dr. Rosen brings deep expertise in the unique challenges facing physicians navigating modern medical practice.
His work focuses on helping physicians navigate burnout, address moral injury, and maintain psychological wellness amid the demands of medical practice. Dr. Rosen’s approach combines evidence-based therapeutic techniques (Acceptance and Commitment Therapy, Cognitive-Behavioral Therapy, moral injury-informed approaches) with an understanding of the discrete, flexible, completely confidential care that physicians require.
References
1. American Medical Association. (2024). Burnout Rate Improving Among Physicians, Though Rates Remain High. Retrieved from https://www.ama-assn.org/press-center/ama-press-releases/burnout-rate-improving-among-physicians-though-rates-remain-high
2. Commonwealth Fund. (2025). Causes and Impacts of Burnout in Primary Care Physicians: 10 Countries Survey. Retrieved from https://www.commonwealthfund.org/publications/surveys/2025/nov/causes-impacts-burnout-primary-care-physicians-10-countries
3. National Center for Biotechnology Information. (2024). Physician Burnout: Evidence-Based Roadmaps to Prioritizing and Supporting Personal Wellbeing. Journal of Healthcare Leadership. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10773242/
4. National Institute for Occupational Safety and Health. (2023). Preventing Burnout Among Healthcare Workers. U.S. Department of Health and Human Services. Retrieved from https://www.cdc.gov/niosh/topics/healthcare/burnout.html
5. Frontiers in Public Health. (2025). Toward Better Prevention of Physician Burnout: Insights from Individual Participant Data Using the MD-Specific Occupational Stressor Index and Organizational Interventions. Retrieved from https://www.frontiersin.org/journals/public-health/articles/10.3389/fpubh.2025.1514706/full
Crisis Resources
If you are experiencing a mental health crisis or having thoughts of suicide, please reach out immediately:
988 Suicide & Crisis Lifeline: Call or text 988
Crisis Text Line: Text HOME to 741741
National Alliance on Mental Illness (NAMI): 1-800-950-NAMI (6264)