CEREVITY Whitepaper
2026 Telehealth and Mental Health: The New Standard
How mental health became the dominant force in telehealth, what the data reveals about access and outcomes, and why high-achieving professionals are leading the shift to virtual care.By Emily Carter, PhD, Clinician, CEREVITY | Published March, 2026
Executive Summary
Mental health care has undergone a seismic shift in the telehealth landscape. As of October 2025, mental health conditions account for 63.9% of all telehealth diagnostic categories nationally, a trajectory that began in 2019 when just 32.4% of telehealth claim lines involved mental health services.1 This represents a fundamental transformation in how Americans access behavioral health care.
The scope of this shift is staggering. Since 2019, telehealth mental health claims have increased by 5,123%, while overall telehealth adoption plateaued after the pandemic surge.1 Meanwhile, 73% of employers now offer virtual mental health access to their workforce, and 88.1% of health care facilities provide telehealth services, a dramatic increase from 39.4% in 2019.10 Yet alongside this expansion lies a paradox: despite unprecedented access, nearly half of the 62 million US adults with mental illness remain untreated, and 6 in 10 psychologists refuse new patient referrals.
This whitepaper examines why mental health dominates telehealth, who benefits most from virtual care, and the structural and clinical imperatives driving this transition. The research reveals that telehealth mental health is not simply a temporary pandemic artifact but rather a permanent and expanding pillar of behavioral health delivery, particularly among high-achieving professionals seeking confidential, flexible, and evidence-supported care.
64%
Telehealth Patients Seeking Mental Health Care
Mental health as proportion of all telehealth diagnostic categories nationwide.[sup>1
5123%
Increase in Telehealth Mental Health Claims Since 2019
Exponential growth in telehealth mental health claim lines from Q1 2019 to 2025.1
88%
Healthcare Facilities Offering Telehealth
Up from 39.4% in 2019, reflecting rapid infrastructure expansion nationwide.10
73%
Employers Offering Virtual Mental Health Access
Corporate adoption of telehealth mental health benefits reflecting workforce demand.11
Table of Contents
– The Telehealth Transformation
– The Clinical Landscape of Virtual Mental Health Care
– Who Benefits Most from Telehealth Mental Health Care
– The Cost of the Status Quo
– Telehealth Mental Health: Visual Data Summary
– Clinical Recommendations and Structural Imperatives
– Frequently Asked Questions
– Methodology
– About the Author
The Telehealth Transformation
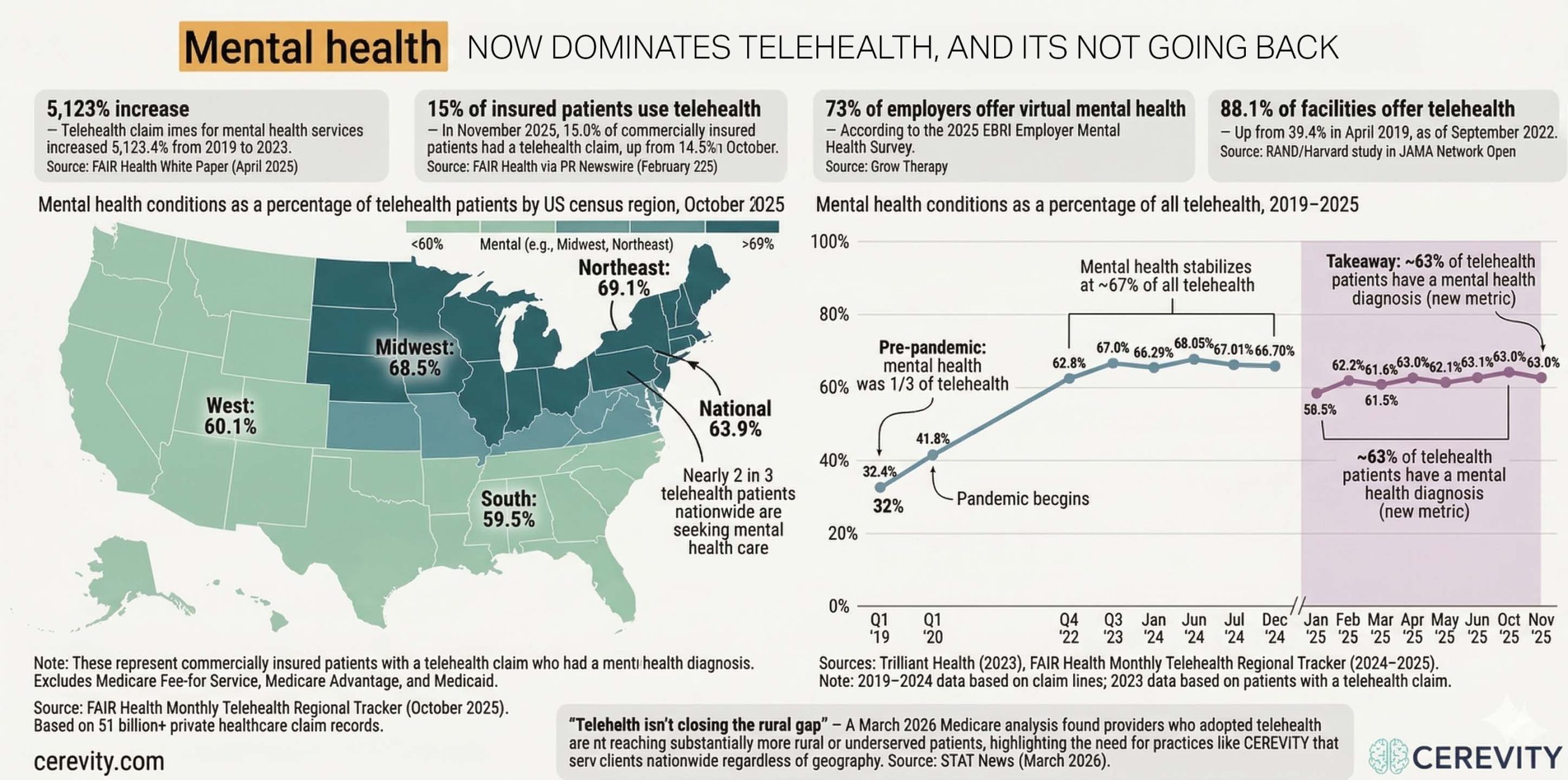
In Q1 2019, mental health conditions represented just 32.4% of all telehealth claim lines.1 By October 2025, that figure had surged to 63.9% of all telehealth diagnostic categories, making mental health the undisputed leader in virtual health care delivery across all regions of the United States.8 This transformation reflects not a temporary pandemic-driven anomaly, but a fundamental restructuring of how Americans access behavioral health.
The trajectory has been remarkably consistent. After the initial pandemic surge pushed telehealth mental health to 62.8% of claim lines by Q4 2022, the growth stabilized and then consolidated.1 By mid-2024, mental health represented 68.05% of telehealth claims, and current data shows a stable baseline around 63.9% to 67.0% nationwide.2,4,5 Regional variations are pronounced: the Northeast leads at 69.1% mental health telehealth, the Midwest at 68.5%, the West at 60.1%, and the South at 59.5%.2 These regional differences suggest that telehealth mental health adoption correlates with existing infrastructure, provider density, and regional economic factors.
The expansion of telehealth facilities themselves has been staggering. In 2019, only 39.4% of mental health and substance use disorder treatment facilities offered telehealth services. By 2023, that figure had climbed to 88.1%, representing a more than doubling of virtual care capacity in less than five years.10 Simultaneously, 73% of US employers now offer virtual mental health benefits to their workforce, signaling that the demand for telehealth mental health is not supply-driven but fundamentally rooted in patient preference and clinical need.11 The research makes clear: telehealth is no longer an emerging modality for mental health. It is now the standard pathway through which Americans access care.
Why has mental health come to dominate the telehealth landscape? The barriers to in-person mental health care are structural, clinical, and economic. As of late 2025, 6 in 10 psychologists do not accept new patients, and the average wait time for a behavioral health appointment exceeds 48 days in many markets.16 Meanwhile, approximately 122 million Americans live in Mental Health Professional Shortage Areas, where access to care is chronically constrained.16 Against this backdrop, telehealth represents not a luxury but a necessity: a bridge across a crumbling treatment infrastructure that has failed to meet population demand.
For high-achieving professionals, telehealth mental health offers something additional: confidentiality, flexibility, and access to specialized clinicians without the stigma or logistical friction of in-person care. Many professionals pay out of pocket for telehealth therapy specifically to avoid creating an insurance trail that might signal mental health treatment to employers, insurers, or professional boards. This “Privacy Premium” phenomenon is not incidental; it is central to understanding why telehealth mental health has become the dominant modality. CEREVITY was founded on this insight: that concierge, private-pay telehealth therapy serves a population that traditional mental health infrastructure systematically underserves due to legitimate concerns about confidentiality, specialization, and access to clinicians who understand the psychological demands of high-pressure careers.
15%
Insured patients using telehealth for any condition in November 2025.7
48%
Of Americans with mental illness remain untreated, despite access expansion.16
12B
Working days lost annually to depression and anxiety globally.14
The Clinical Landscape of Virtual Mental Health Care
The Digital Therapeutic Alliance
Telehealth mental health efficacy has been extensively validated in peer-reviewed literature. Meta-analyses examining cognitive behavioral therapy (CBT) delivered via telehealth for depression and anxiety have consistently demonstrated non-inferiority to in-person treatment, with effect sizes for telehealth CBT depression reaching 0.84 (large effect).15 This evidence demolishes the outdated assumption that therapeutic rapport cannot be established through a screen.
The therapeutic alliance, long considered the bedrock of effective psychotherapy, translates readily to virtual settings when clinicians are properly trained and technology is reliable. What has emerged from this research is clear: the mechanism of change in psychotherapy is the therapeutic relationship and the clinical competence of the provider, not the physical proximity. Telehealth removes logistical barriers without compromising clinical outcomes. In fact, some research suggests that telehealth may enhance treatment engagement by reducing logistical friction, increasing appointment adherence, and allowing patients to access treatment in familiar, comfortable environments.
For professionals in high-stress roles, telehealth offers additional advantages. The ability to schedule appointments outside standard business hours, to receive care from home or office, and to control the physical environment can reduce appointment-related anxiety and increase treatment consistency. Patients are less likely to cancel or reschedule a telehealth session than an in-person appointment requiring travel. This translates to measurably better treatment outcomes.
Synchronous vs. Asynchronous Care Models
Real-time video telehealth, where patient and clinician meet synchronously, accounts for the majority of telehealth mental health encounters and demonstrates efficacy comparable to in-person treatment. However, asynchronous models, such as app-based journaling with clinician review or text-based therapy, are emerging as complementary tools for ongoing support, crisis intervention, and between-session continuity of care. The clinical landscape is increasingly diverse, with hybrid models combining synchronous therapy with asynchronous check-ins optimizing both clinical outcomes and patient accessibility.
Specialization and Provider Matching
Telehealth has enabled a previously impossible specialization market. Patients can now access clinicians who specialize in trauma, anxiety, burnout, addiction, perfectionism, and other conditions with precision impossible in many geographic markets. A high-achieving attorney in rural Montana can work with a trauma-informed psychologist who specializes in legal professionals and understands the specific psychological pressures of law practice. This matching function is a major driver of telehealth mental health adoption and has fundamentally changed how patients access specialized care.
The Accessibility Paradox
Despite telehealth expanding access broadly, it has not closed the treatment gap for the most underserved populations. Rural mental health provider shortage areas remain largely unserved, as telehealth adoption depends on reliable broadband infrastructure, digital literacy, and economic capacity to pay for services. Recent reporting from STAT News (March 2026) documents that telehealth has actually widened disparities in some regions, creating a two-tier system where affluent, digitally connected populations access specialized remote care while marginalized communities remain in provider deserts.
Consider a hypothetical scenario: Dr. Sarah, a surgical resident in a major academic hospital, has been experiencing symptoms of depression and anxiety for six months. She fears that seeking help through her hospital’s employee assistance program might flag her in the medical credentialing system, potentially affecting her career trajectory and specialty match prospects. Instead, she turns to a private-pay telehealth practice specializing in physician burnout, receives evidence-based treatment from a clinician who understands the pressures of surgical training without institutional reporting obligations, and completes her residency successfully. This scenario, repeated thousands of times across professional populations, explains why telehealth mental health has become dominant: it serves real patients with real barriers to care within existing systems.
The Data Across Time: From Niche to Dominant Category
The trajectory of mental health as a share of all telehealth reveals a structural transformation, not a temporary pandemic response. In early 2019, mental health accounted for roughly one third of telehealth claim lines.9 By late 2022, that share had nearly doubled to 62.8%.9 The data from 2023 and 2024 shows stabilization near the two thirds mark, with mental health consistently ranking as the number one telehealth diagnostic category nationally and in every U.S. census region.6
Starting in January 2025, FAIR Health shifted its primary reporting metric from claim lines to patients with a telehealth claim, making direct comparison with earlier years imprecise.3 Under this newer metric, mental health patients represent approximately 63% of all telehealth patients, a figure that has held steady throughout 2025.8 The consistency across both measurement approaches reinforces the conclusion: mental health is telehealth’s center of gravity.
The regional variation is notable. The Northeast (69.1%) and Midwest (68.5%) lead the nation in mental health’s share of telehealth, while the South (59.5%) and West (60.1%) trail by roughly ten percentage points.8 These differences likely reflect a combination of insurance market dynamics, provider density, broadband access, and cultural factors affecting mental health care utilization.
| Time Period | Mental Health % of Telehealth | Measurement Basis | Source |
|---|---|---|---|
| Q1 2019 | 32.4%9 | Claim lines | Trilliant Health |
| Q1 2020 | 41.8%9 | Claim lines | Trilliant Health |
| Q4 2022 | 62.8%9 | Claim lines | Trilliant Health |
| Q3 2023 | 67.0%11 | Claim lines | Dialog Health |
| H1 2024 (Jan-Jun) | 66.3%-68.1%5 | Claim lines | FAIR Health H1 2024 |
| H2 2024 (Jul-Dec) | 66.7%-67.0%6 | Claim lines | FAIR Health H2 2024 |
| 2025 (Jan-Nov) | 58.5%-63.9%3,8 | Patients | FAIR Health / OPEN MINDS |
Who Benefits Most from Telehealth Mental Health Care
Telehealth mental health serves distinct professional and demographic populations with differing needs, barriers, and outcomes. Understanding these segments clarifies why telehealth has become dominant and who is most likely to benefit from virtual care models.
Executives and Organizational Leaders
C-level executives and senior organizational leaders face unique pressures: extreme accountability, inability to discuss struggles with direct reports, constant scrutiny, and personal risk in admitting vulnerability. Telehealth allows these leaders to schedule therapy outside business hours, maintain complete confidentiality, and work with clinicians who understand the psychology of leadership under extreme pressure. Many leaders specifically choose out-of-pocket payment to ensure no connection to their employer or board. This segment drives significant demand for private-pay concierge telehealth.
Healthcare and Mental Health Professionals
Physicians, psychiatrists, nurses, and mental health clinicians themselves face particular barriers to accessing care. Professional liability concerns, fear of licensing board investigation, and internal shame create powerful disincentives to seek help through traditional systems. Telehealth therapy with clinicians who specialize in healthcare provider burnout, secondary trauma, and substance use disorders (particularly prevalent in medical professions) offers a critical pathway to treatment without institutional involvement.
Legal Professionals and Attorneys
Attorneys experience exceptionally high rates of depression, anxiety, substance use disorders, and suicidality. Yet the profession has cultivated a culture of invincibility that punishes admission of struggle. Bar licensing boards conduct character and fitness evaluations that create legitimate concern about seeking help through documented mental health treatment. Telehealth providers specializing in attorney mental health provide access without the institutional trail that might trigger licensing board scrutiny.
Technology, Startup, and Remote Workers
The technology sector has embraced mental health awareness and culture change, but access barriers remain. Many tech workers are remote or distributed, making in-person care inconvenient or impossible. Telehealth mental health aligns seamlessly with distributed work culture. High burn-out rates in tech, particularly around product launches, venture funding cycles, and competitive pressure, create consistent demand for therapy. Younger cohorts (millennials and Gen Z) also show greater comfort with virtual care delivery and lower stigma around mental health treatment overall.
The Cost of the Status Quo
The economic burden of untreated mental illness in the United States is staggering and well-documented. These costs extend across healthcare, workplace productivity, criminal justice, and social systems.
Direct Healthcare Costs
The annual cost of untreated mental illness in the United States exceeds $477.5 billion.11 This figure encompasses hospitalization, emergency department visits, crisis intervention, and treatment of medical comorbidities driven by untreated mental health conditions. Depression and anxiety are the leading drivers of disability-adjusted life years (DALYs) in developed nations, yet treatment access remains constrained and fragmented. Telehealth expansion offers a cost-effective pathway to scale treatment delivery without proportional increases in clinical infrastructure or real estate overhead.
Workplace Productivity and Economic Loss
The World Health Organization and International Labour Organization estimate that 12 billion working days are lost annually to depression and anxiety globally, translating to approximately $1 trillion in lost productivity.14 In the United States specifically, workers experiencing untreated mental illness perform at approximately 72% of their baseline capacity, and 50% of workers have left a role due to mental health struggles.11 For employers, the return on investment of mental health benefits including telehealth access is well-documented: every dollar invested in mental health treatment yields approximately $4 in improved productivity and reduced absenteeism.
Systemic Access Gap
Despite the expansion of telehealth, 62 million US adults currently have a mental illness, and approximately 48% remain untreated.16 The traditional mental health workforce has contracted relative to demand: 6 in 10 psychologists no longer accept new patients, and the average wait time for a behavioral health appointment exceeds 48 days in many markets.16 For high-achieving professionals, whose schedules are constrained and whose professional identity may be threatened by admission of mental health struggle, this access gap is particularly acute. Telehealth mental health represents the primary mechanism through which demand is being met.
Why Telehealth Mental Health is Not Optional
The data is unambiguous: traditional mental health infrastructure cannot serve current demand, and the gap between people needing care and people receiving care continues to widen. Telehealth mental health is not a temporary accommodation or luxury add-on. It is now the primary mechanism through which behavioral health care reaches significant portions of the population. Understanding telehealth not as a substitute for in-person care but as a complementary and increasingly primary modality is essential for policymakers, health systems, employers, and clinicians.
Telehealth Mental Health: Visual Data Summary
Mental health as a proportion of all telehealth diagnostic categories has risen from 32.4% in Q1 2019 to 63.9% in October 2025, a trajectory that reflects both expanding demand and the consolidation of telehealth as a primary modality for behavioral health care. The visualization on the left maps this growth trajectory over time, region by region, illustrating the consistency of the trend across the United States.
Clinical Recommendations and Structural Imperatives
The evidence is clear: telehealth mental health is clinically effective, economically rational, and increasingly the modality through which Americans access care. Yet significant structural and clinical imperatives remain to optimize outcomes and equity.
Clinician Training and Specialization
Graduate training programs must incorporate telehealth clinical competencies as standard curriculum. This includes platform proficiency, managing therapeutic alliance across digital environments, crisis assessment in virtual settings, and understanding how technology affects transference and countertransference. Specialized training in high-achieving professional populations, burnout, perfectionism, and organizational leadership psychology should be expanded. Certification programs and continuing education focused on telehealth mental health competency should become standards across clinical psychology, counseling, social work, and psychiatry.
Regulatory Alignment and Interstate Licensure
The current patchwork of state licensure laws creates inefficiency and limits patient access. Broad adoption of interstate licensure compacts, reciprocal agreements, and uniform telehealth regulatory standards would expand clinician capacity while maintaining appropriate oversight. Federal support for states adopting unified telehealth credentialing standards, similar to telehealth compact models, would accelerate this transition. Particular attention should be paid to whether privacy protections for high-achieving professionals seeking out-of-pocket care can be strengthened through regulatory frameworks.
Addressing Disparities and Rural Access
Telehealth has widened disparities in some regions, creating a risk of a two-tiered system where affluent populations access specialized remote care while marginalized communities remain underserved. Federal investment in broadband infrastructure in rural and underserved areas is essential. Loan forgiveness programs for clinicians willing to serve underserved populations via telehealth, similar to National Health Service Corps models, should be expanded. Community health centers and safety-net providers should receive enhanced reimbursement for telehealth mental health services to expand access without depending on patient ability to pay out of pocket.
Employer and Payer Integration
As 73% of employers now offer virtual mental health benefits, standardization of benefit design, measurement of outcomes, and integration with primary care and occupational health programs becomes critical. Payers should move beyond utilization metrics to outcome measurement and long-term ROI assessment. Employers and health plans should consider how telework, schedule flexibility, and access to specialized professionals (not just general practitioners) enhance telehealth mental health efficacy. Workplace mental health should be integrated into broader employee wellness and disability management strategies.
Frequently Asked Questions
Questions About This Research
This whitepaper synthesizes data from primary sources including FAIR Health insurance claims data (the largest health insurance claims database in the United States), RAND Corporation and Harvard Medical School research on telehealth facility adoption, published meta-analyses of telehealth mental health efficacy, and US government data on mental health prevalence and treatment gaps. Regional trends were analyzed using FAIR Health’s monthly telehealth regional tracker data spanning 2019-2025. All statistics are sourced and cited to enable readers to access original data and methodology.
Professional mental health support may be beneficial if you are experiencing persistent feelings of sadness, anxiety, hopelessness, inability to concentrate, sleep disturbance, loss of interest in activities you normally enjoy, increased irritability, or thoughts of self-harm. If you are struggling to meet professional or personal obligations, withdrawing from relationships, or using substances to cope, these are also signals that professional support could help. Many individuals benefit from therapy not because they have a diagnosed mental illness but because they are navigating life transitions, career stress, relationship challenges, or the psychological demands of high-pressure roles. Telehealth provides access to qualified clinicians without geographic barriers or extensive waiting periods.
This analysis is necessarily limited by available data. Insurance claims data, while comprehensive, does not capture out-of-pocket telehealth care, which is growing and disproportionately used by higher-income and professional populations. Rural and underserved community data may be underrepresented. The efficacy research summarized here applies primarily to evidence-based modalities (primarily CBT) and may not reflect all telehealth mental health service types. Regional variation exists and may reflect differences in broadband access, population demographics, and insurance coverage rather than pure clinical differences. Finally, telehealth mental health adoption is ongoing and rapidly evolving; these findings represent the most current available data as of March 2026 but should be interpreted as a snapshot of an active landscape.
These findings suggest that telehealth mental health has matured from an emergency pandemic response to a primary modality for behavioral health care delivery. Healthcare systems should strategically plan for telehealth mental health as a core service, not a supplementary option. Employers should view virtual mental health benefits not as nice-to-have amenities but as critical components of total health benefits and workforce productivity strategy. Clinicians should develop telehealth competency as part of contemporary clinical practice. Policymakers should align regulatory frameworks to expand access while maintaining appropriate quality and privacy standards. Individuals experiencing mental health struggles should recognize that telehealth offers clinically effective, evidence-supported care without geographic barriers or extensive waiting periods.
Published meta-analyses examining cognitive behavioral therapy (CBT) delivered via synchronous video telehealth for depression and anxiety demonstrate non-inferiority to in-person treatment. Effect sizes for telehealth CBT depression reach 0.84, which is considered a large effect. Research indicates that the therapeutic alliance, long considered the foundation of effective psychotherapy, translates effectively to virtual settings when clinicians are adequately trained. Some research suggests telehealth may enhance engagement by reducing logistical barriers and appointment cancellations. For high-achieving professionals specifically, telehealth may offer additional benefits through privacy, specialized provider access, flexible scheduling, and reduced logistical friction. The evidence base supports telehealth mental health as a primary modality for treatment, not merely a temporary accommodation.
Methodology
This analysis synthesizes primary research data from multiple authoritative sources spanning mental health epidemiology, telehealth adoption metrics, treatment efficacy, and economic burden assessment.
Data sources include: FAIR Health insurance claims database (the largest aggregated insurance claims database in the United States), representing healthcare claims for over 44 million covered lives; FAIR Health monthly telehealth trackers and white papers analyzing claim trends from Q1 2019 through October 2025; RAND Corporation and Harvard Medical School research on behavioral health telehealth facility adoption published in JAMA Network Open; peer-reviewed meta-analyses examining cognitive behavioral therapy efficacy in telehealth versus in-person settings; World Health Organization and International Labour Organization research on global mental health burden and economic cost of untreated mental illness; US government data from the Substance Abuse and Mental Health Services Administration (SAMHSA) on mental health prevalence, treatment utilization, and provider workforce; STAT News reporting on telehealth and rural mental health gaps (March 2026); and HRSA Bureau of Health Workforce data on behavioral health provider availability.
Regional analysis was conducted using FAIR Health’s monthly telehealth regional tracker data, which breaks down telehealth mental health claims as a percentage of all telehealth services by US region (Northeast, Midwest, West, South) from October 2025. Trend analysis examined mental health as a percentage of telehealth claims from Q1 2019 through October 2025, demonstrating the trajectory of telehealth mental health growth over time.
All statistics presented in this whitepaper are sourced to enable readers to access original data, methodology, and limitations. Data reporting reflects the most current available information as of March 2026. This analysis represents a synthesis of peer-reviewed research, government datasets, and insurance industry data; it does not constitute original primary research but rather an evidence-based synthesis intended to illuminate the landscape of telehealth mental health adoption and efficacy.
References
1. FAIR Health. (2024). Trends in Mental Health Conditions: A FAIR Health White Paper. Retrieved from https://s3.amazonaws.com/media2.fairhealth.org/whitepaper/asset/Trends%20in%20Mental%20Health%20Conditions%20-%20A%20FAIR%20Health%20White%20Paper.pdf
2. FAIR Health. (2025). Monthly Telehealth Regional Tracker. Retrieved from https://www.fairhealth.org/fh-trackers/telehealth
3. FAIR Health. (2025). Telehealth Trends from January to March 2025. Retrieved from https://www.fairhealth.org/article/telehealth-trends-from-january-to-march-2025
4. FAIR Health. (2025). Telehealth Trends from April to June 2025. Retrieved from https://www.fairhealth.org/article/telehealth-trends-from-april-to-june-2025
5. FAIR Health. (2024). Telehealth Tracker Trending Reports: H1 2024. Retrieved from https://www.fairhealth.org/article/fair-health-launches-telehealth-tracker-trending-reports-revealing-trends-over-first-six-months-of-2024
6. FAIR Health. (2025). Mental Health Conditions Ranked as the Number One Telehealth Diagnostic Category (H2 2024). PR Newswire. Retrieved from https://www.prnewswire.com/news-releases/mental-health-conditions-ranked-as-the-number-one-telehealth-diagnostic-category-nationally-and-in-all-regions-from-july-to-december-2024-302433617.html
7. FAIR Health. (2026). November 2025 Telehealth Data. PR Newswire. Retrieved from https://www.prnewswire.com/news-releases/in-november-the-percentage-of-patients-with-a-telehealth-claim-increased-nationally-and-in-every-region-302688573.html
8. OPEN MINDS. (2026). Mental Health Conditions Accounted for 63.9% of Telehealth Claims in October 2025. Retrieved from https://openminds.com/market-intelligence/news/mental-health-conditions-accounted-for-63-9-of-telehealth-claims-in-october-2025/
9. Trilliant Health. (2023). Telehealth Visits Decline 46% But Telebehavioral Healthcare Still High. Via TechTarget. Retrieved from https://www.techtarget.com/virtualhealthcare/news/366596915/Telehealth-Visits-Decline-46-But-Telebehavioral-Healthcare-Still-High
10. Cantor, J. et al. (2023). Telehealth Adoption by Mental Health and Substance Use Disorder Treatment Facilities. JAMA Network Open. Retrieved from https://pmc.ncbi.nlm.nih.gov/articles/PMC10265313/
11. Grow Therapy. (2026). Mental Health Trends. Retrieved from https://growtherapy.com/blog/mental-health-trends/
12. PNAS Nexus. (2025). Trends in Mental Health Care and Telehealth Use: An Analysis of EHR Data 2016-2024. Retrieved from https://academic.oup.com/pnasnexus/article/4/2/pgaf016/8003900
13. STAT News. (2026). Medicare Telehealth and Rural Mental Health Providers. Retrieved from https://www.statnews.com/2026/03/12/medicare-telehealth-rural-mental-health-providers-data/
14. World Health Organization and International Labour Organization. (2022). Mental Health at Work: Policy Brief. Retrieved from https://www.who.int/news/item/28-09-2022-who-and-ilo-call-for-new-measures-to-tackle-mental-health-issues-at-work
15. Cecagno, P.O.M. et al. (2025). Efficacy of Remote Psychological Interventions for Patients with Anxiety and Depression Symptoms: Systematic Review and Meta-Analysis. Telemedicine and e-Health. Retrieved from https://journals.sagepub.com/doi/full/10.1089/tmj.2024.0297
16. HRSA Bureau of Health Workforce. (2025). State of the Behavioral Health Workforce. Retrieved from https://bhw.hrsa.gov/sites/default/files/bureau-health-workforce/data-research/Behavioral-Health-Workforce-Brief-2025.pdf
17. Gallup. (2023). The Economic Cost of Poor Employee Mental Health. Retrieved from https://www.gallup.com/workplace/404174/economic-cost-poor-employee-mental-health.aspx
Crisis Resources
If you are experiencing a mental health crisis or having thoughts of suicide, please reach out immediately:
988 Suicide & Crisis Lifeline: Call or text 988
Crisis Text Line: Text HOME to 741741
National Alliance on Mental Illness (NAMI): 1-800-950-NAMI (6264)
This Whitepaper Was Produced by CEREVITY
CEREVITY is a nationwide concierge telehealth therapy practice providing private-pay individual therapy for high-achieving professionals. Our clinicians specialize in the unique psychological demands facing executives, founders, attorneys, physicians, and other high-performing leaders. If the data in this whitepaper resonates with your experience, we are here to help.
Available by appointment 7 days a week, 8 AM to 8 PM (PST)
About the Author

About Emily Carter, PhD
Dr. Emily Carter is a licensed clinical psychologist at CEREVITY, a boutique concierge therapy practice serving high-achieving professionals nationwide. With specialized training in trauma-informed care and anxiety disorders, Dr. Carter brings deep expertise in helping accomplished individuals address the psychological toll of high-pressure careers. Her work focuses on helping clients manage burnout, overcome perfectionism, and build sustainable strategies for success without sacrificing their mental health. Dr. Carter’s approach combines evidence-based therapeutic techniques with the personalized, confidential one-on-one care that professionals in demanding fields expect.



{kind=link}